


Drug-Induced Choking: How Common Senior Medications Cause Swallowing Risk (2026 Family Guide)
Quick Answer: Many common medications prescribed to seniors increase choking risk by causing dry mouth, slowing swallowing reflexes, or directly impairing throat muscle coordination. Per FDA Adverse Event Reporting System (FAERS) data and the 2023 AGS Beers Criteria, 17+ drug categories carry documented dysphagia (swallowing disorder) signals in adults 65+. Antipsychotics (Abilify, Risperdal), benzodiazepines (Xanax, Valium), and anticholinergics top the list. With 35.9% of frail elderly patients having dysphagia (often medication-related), and polypharmacy a major risk factor, every adult child should review their parent's medication list. The NovaCare Anti-Choking Device ($63.98) — Bureau Veritas tested with verified 70 kPa suction — provides emergency response when medication-induced swallowing impairment leads to choking. Save #156 (Harold B., 78) and Save #162 (Dorothy F., 72) document senior self-rescue success.
Your father started a new medication last month. Yesterday at dinner, you noticed his voice sounded "wet" after he drank water. Last week, his caregiver mentioned he's been coughing during meals. You assumed it was a cold.
It might be his medication.
This is the conversation no one — including most primary care doctors — will start with you. But the data is clear: medications are a leading cause of dysphagia (swallowing disorders) in seniors, and dysphagia is the gateway to choking emergencies. This guide explains which medications carry the highest risk, what to watch for, and what every adult child needs to do.
Section 1: Understanding Drug-Induced Dysphagia (5 Questions)
Q1: How can medications cause choking risk?
Medications affect swallowing through several mechanisms:
- Dry mouth (xerostomia) — Reduces saliva needed to safely move food
- Sedation — Slows protective swallowing reflexes
- Muscle coordination impairment — Affects throat muscle synchronization
- Cognitive effects — Reduces awareness during eating
- Direct esophageal effects — Some drugs cause inflammation
- Cumulative anticholinergic burden — Multiple medications compound risk
Per peer-reviewed pharmacovigilance research using the FDA Adverse Event Reporting System (FAERS) database, dopamine-blocking drugs (especially antipsychotics) are the primary contributors to medication-related aspiration pneumonia risk in elderly populations.
Q2: How common is medication-induced dysphagia?
More common than most families realize. Per peer-reviewed clinical studies:
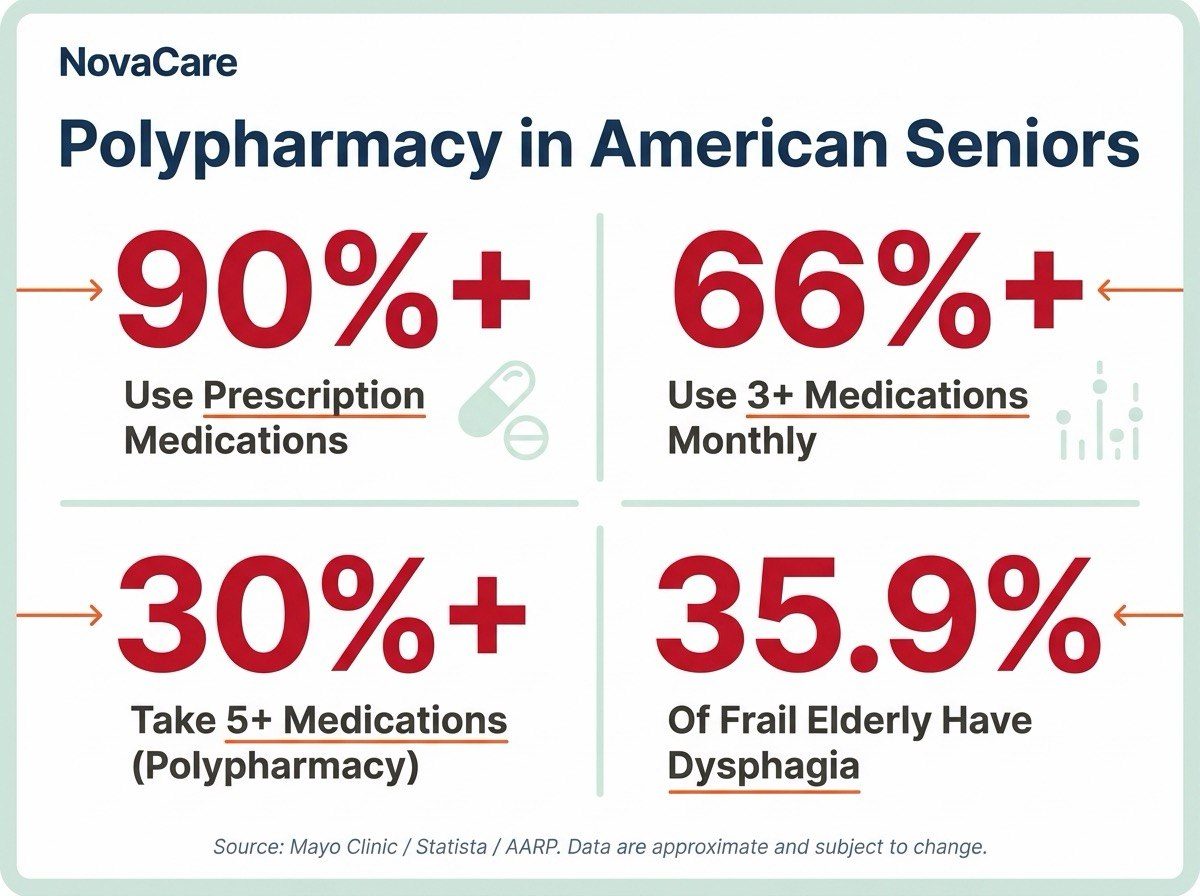
- 35.9% of frail elderly patients have dysphagia (Mianyang Hospital study, 2024)
- Polypharmacy (multiple medications) is one of the top dysphagia risk factors
- 91.7% of pneumonia patients 70+ have dysphagia (StatPearls/NIH)
- 50% of these patients experience silent aspiration
- Many cases are medication-induced and reversible with medication adjustment
The intersection of aging-related swallowing changes + medication side effects creates a dangerous compound effect.
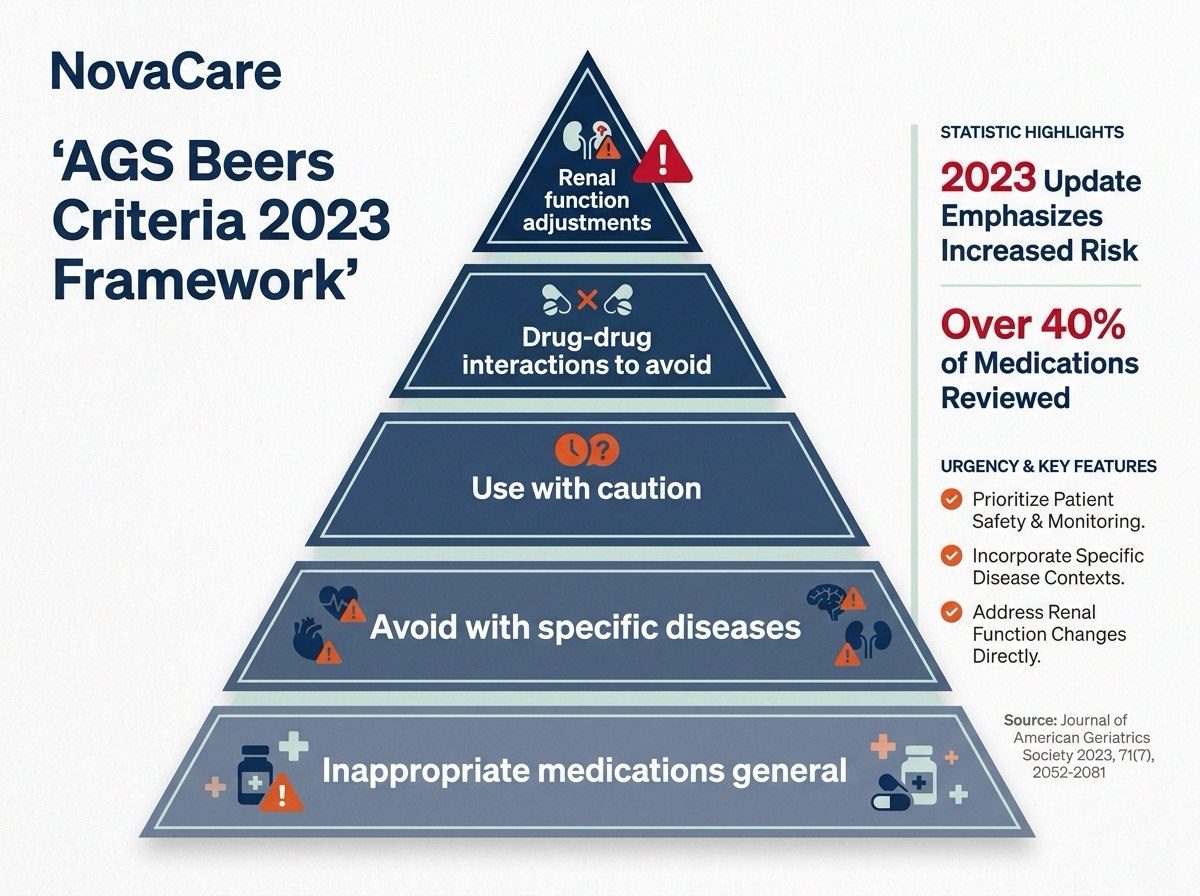
Q3: What is the AGS Beers Criteria?
The American Geriatrics Society (AGS) Beers Criteria® is the gold-standard reference for medications adults 65+ should avoid or use with caution. The 2023 edition (most recent) was published May 4, 2023, in the Journal of the American Geriatrics Society.
The criteria identifies "Potentially Inappropriate Medications" (PIMs) based on rigorous evidence review by an expert panel. With more than 90% of older adults using at least one prescription and more than 66% using three or more medications monthly, this list is critical for family safety planning.
Multiple medications on the Beers Criteria are linked to choking risk through their dysphagia-related mechanisms.
Q4: What's "polypharmacy" and why does it matter?
Polypharmacy = taking 5 or more medications simultaneously. It's extremely common in seniors:
- 66%+ of adults 65+ take 3+ medications
- 30%+ take 5+ medications
- 15%+ take 10+ medications
The danger: each medication may seem individually safe, but combinations create cumulative effects. Per peer-reviewed research, polypharmacy is an independent risk factor for dysphagia with each additional medication increasing risk.
Critical concern — cumulative anticholinergic burden: Many over-the-counter medications (Benadryl, sleep aids), antidepressants, and bladder control medications all have anticholinergic effects. Combined, they can dramatically impair swallowing.
Q5: How does medication-induced dysphagia lead to choking emergencies?
The progression is often gradual:
- New medication started → mild dry mouth, slight cough during meals
- Mild symptoms ignored or attributed to "aging"
- Silent aspiration episodes begin (no obvious symptoms)
- Aspiration pneumonia may develop (often misdiagnosed)
- Complete obstruction emergency occurs unpredictably
- Without equipment, 4-minute brain damage window
This is why both Save #156 (Harold B., 78) and Save #162 (Dorothy F., 72) involved seniors with no known dysphagia diagnosis who suddenly faced complete obstruction emergencies. Many seniors with medication-induced dysphagia are walking around without a diagnosis.
Section 2: High-Risk Medication Categories (5 Questions)
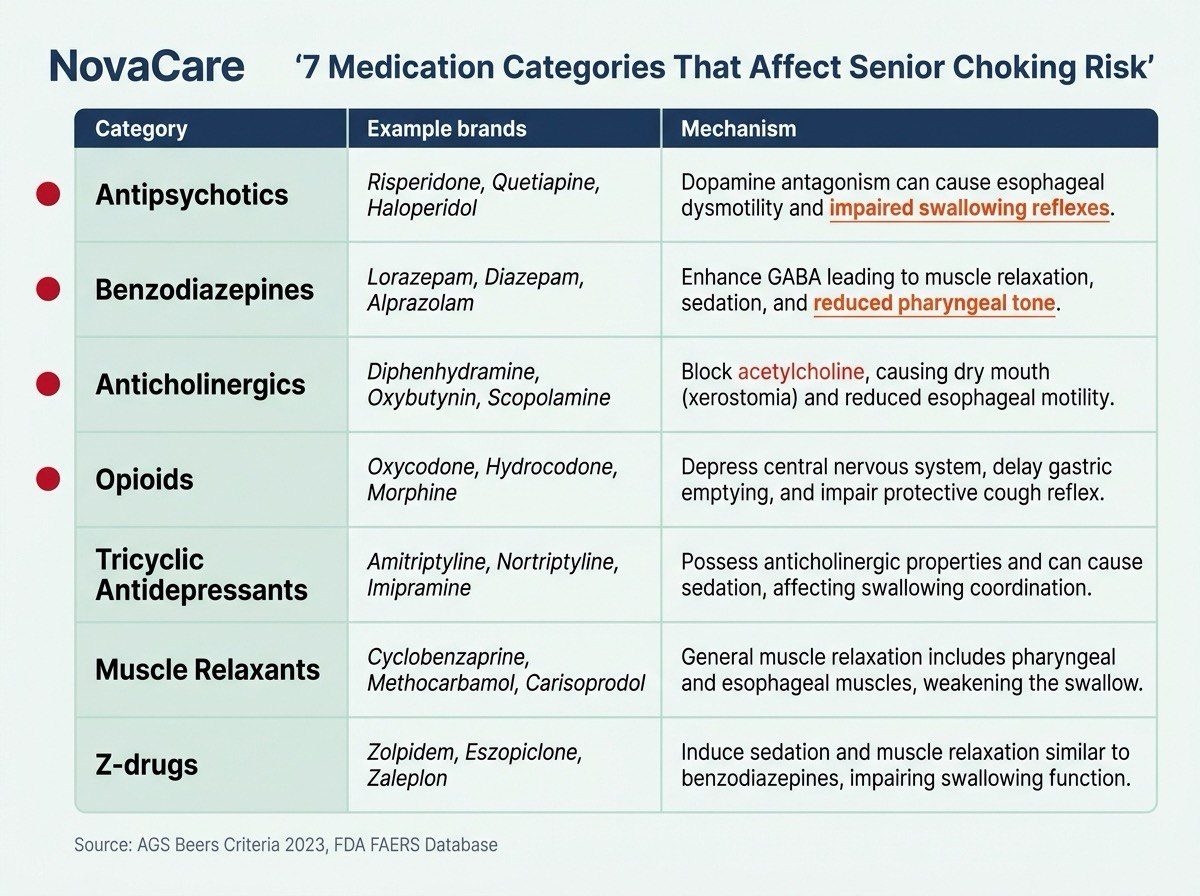
Q6: Which medication categories pose the highest choking risk?
| Category | Examples | Mechanism |
|---|---|---|
| Antipsychotics | Abilify, Risperdal, Zyprexa, Seroquel, Haldol | Dopamine blocking → swallowing impairment |
| Benzodiazepines | Xanax, Valium, Ativan, Klonopin | Sedation → reduced reflexes |
| Anticholinergics | Benadryl, Tylenol PM, oxybutynin | Dry mouth + cognitive effects |
| Opioids | OxyContin, Vicodin, Tramadol | Sedation + reduced cough reflex |
| Tricyclic Antidepressants | Amitriptyline, nortriptyline | Anticholinergic + sedation |
| Muscle Relaxants | Cyclobenzaprine, methocarbamol | Muscle weakness + sedation |
| Z-drugs | Ambien, Lunesta, Sonata | Sedation, especially in elderly |
Multiple of these are on the AGS Beers Criteria as Potentially Inappropriate Medications.
Q7: What about antipsychotics specifically?
Antipsychotics carry the highest documented choking risk among psychiatric medications:
- Per CDC data (2009-2013), schizophrenia patients have a 2.66% choking death rate — among the highest of any condition
- Antipsychotics block dopamine pathways involved in swallowing coordination
- Both first-generation (Haldol) and second-generation (Abilify, Zyprexa) carry risk
- Risk is dose-dependent and increases with combination therapy
- Often prescribed off-label for dementia behavioral symptoms (high concern)
If your senior parent is on antipsychotics for any reason — especially for dementia behaviors — this warrants urgent swallowing evaluation.
Q8: Are sleep aids safe for seniors?
Most are NOT, per AGS Beers Criteria:
- Benzodiazepines (Xanax, Valium, Ativan) — Listed as Avoid in adults 65+
- Z-drugs (Ambien, Lunesta) — Listed as Avoid for chronic use
- Antihistamine sleep aids (Tylenol PM, ZzzQuil) — Strong anticholinergic, Avoid
- Tricyclic antidepressants used for sleep — Avoid in older adults
The double risk: nighttime sedation + reduced cough reflex during sleep = ideal conditions for silent aspiration of saliva → aspiration pneumonia.
If your senior parent uses any sleep aid, especially OTC products, discuss alternatives with their physician. Many primary care doctors don't review the Beers Criteria when prescribing.
Q9: What about Parkinson's medications? (The paradox)
Parkinson's medications create a complex situation:
- Parkinson's itself causes dysphagia in 60-80% of advanced cases (AAO-HNS Bulletin)
- Medications (Levodopa, dopamine agonists) help motor symptoms
- BUT during "off periods" when medication wears off, swallowing dramatically worsens
- Some Parkinson's medications themselves cause additional swallowing issues
- Polypharmacy is common (Parkinson's + other conditions)
For Parkinson's families, equipment readiness is essential. See our dedicated Parkinson's anti-choking guide for specific recommendations.
Q10: Are there specific medication combinations that compound risk?
The AGS Beers Criteria specifically warns about cumulative anticholinergic burden:
- 2+ anticholinergic medications together = severely impaired swallowing
- Sedative + sedative combinations
- Anticholinergic + sedative combinations
- Multiple psychiatric medications
Common dangerous combinations:
- Bladder medication (oxybutynin) + sleep aid (Tylenol PM) = double anticholinergic
- Antidepressant + antipsychotic + sleep aid = triple sedation
- Antihistamine allergy med + bladder med = double anticholinergic
If your parent takes 5+ medications, request a pharmacist review specifically for cumulative effects.
Section 3: Recognizing Drug-Induced Symptoms (5 Questions)
Q11: How do I tell if a new medication is affecting my parent's swallowing?
Watch for these symptoms within 1-4 weeks of starting any new medication:
- Wet/gurgly voice after drinking or eating
- Increased coughing during meals
- "Stuck" sensation in throat
- Avoiding certain foods they used to enjoy
- Increased dry mouth or thick saliva
- Weight loss over weeks/months
- Confusion during meals
- Pocketing food in cheeks
If symptoms appear within 4 weeks of medication change, the medication is the prime suspect.
Q12: Why don't doctors warn about these effects?
Several reasons:
- Primary care doctors juggle many concerns per visit
- The AGS Beers Criteria isn't routinely reviewed in primary care
- Dysphagia symptoms develop gradually (not at prescribing visit)
- Many patients don't volunteer mild symptoms
- Pharmacist counseling is often brief
- Side effect lists are extensive (dysphagia gets buried)
The responsibility often falls to family members to monitor and advocate.
Q13: My parent's medication list seems risky — what should I do?
Step-by-step action plan:
- Document the list — All prescriptions, OTC medications, supplements
- Cross-reference with AGS Beers Criteria — Available at AGS website
- Schedule pharmacist consultation — Ask specifically about cumulative effects
- Request medication review — Many insurance plans cover this
- Bring symptoms list — Document any swallowing concerns
- Request swallowing evaluation — Speech-language pathologist
- Discuss alternatives — Many medications have safer alternatives for elderly
Don't accept "everything looks fine" without a real review of the cumulative anticholinergic burden.
Q14: Are there safer alternatives for common conditions?
Often yes:
| For This Condition | Avoid (per Beers) | Safer Alternative |
|---|---|---|
| Insomnia | Benzodiazepines, Z-drugs | Cognitive behavioral therapy, melatonin (low dose) |
| Allergies | Diphenhydramine (Benadryl) | Loratadine, cetirizine |
| Bladder urgency | Oxybutynin | Mirabegron, behavioral therapy |
| Anxiety | Long-term benzodiazepines | SSRIs, therapy, short-term only |
| Pain | Long-term opioids | Topical NSAIDs, physical therapy |
| Depression | Tricyclic antidepressants | SSRIs, SNRIs |
Discuss alternatives with the prescribing physician. Don't stop medications abruptly.
Q15: What if my parent refuses to discuss their medications?
Common situation. Approaches that work:
- Frame it as "let's just check with pharmacist" (less threatening)
- Use specific symptoms ("Mom, you've been coughing more — let's just ask")
- Bring it up at routine doctor visit
- Suggest medication review as preventive care
- Share specific Beers Criteria information
- Frame around independence ("we want to keep you independent")
Many seniors value the relationship with their doctor. Frame the review as advocacy, not interference.
Section 4: Comparison with Other Choking Devices (5 Questions)
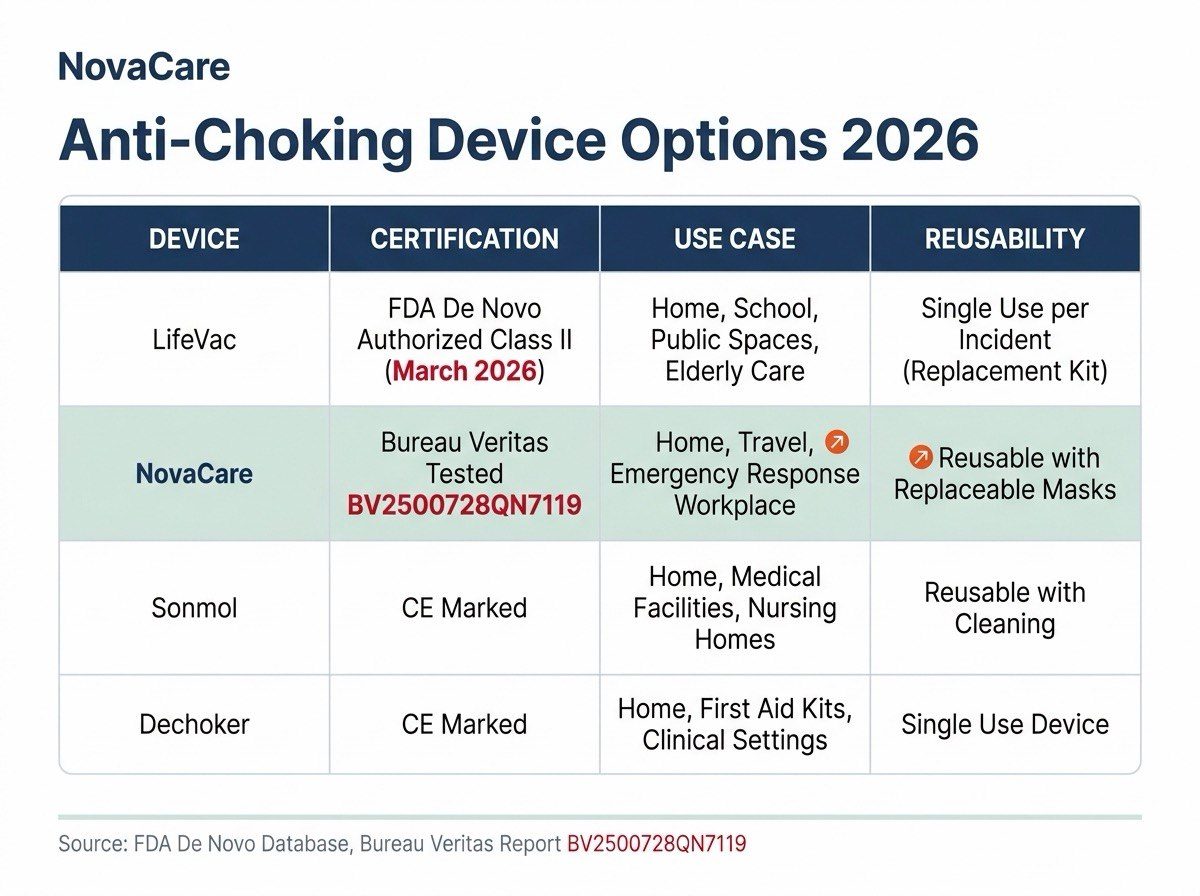
Q16: How does NovaCare compare to other anti-choking devices?
For families managing medication-related choking risks, equipment matters. The major options in 2026:
| Device | Regulatory Status | Use Case | Reusability |
|---|---|---|---|
| LifeVac | FDA De Novo Authorized (March 2026) | Bystander-administered | Single-use |
| NovaCare | Bureau Veritas Tested (Report BV2500728QN7119) | Self-rescue capable | Reusable |
| Sonmol | Various | Wall-mounted, 5-step | Reusable |
| Dechoker | Multiple FDA actions | Tube-based | Reusable |
Q17: What's special about LifeVac?
LifeVac became the first FDA De Novo Authorized anti-choking device on March 4, 2026, classified as a Class II medical device for second-line treatment after standard choking protocols fail.
LifeVac specifications:
- Plunger-style mechanism
- Two-handed operation
- Single-use (must replace after use)
- $59-99 price range
- Designed for bystander rescue
- Multiple mask sizes for different ages
LifeVac is excellent for households with capable bystanders nearby — but its design makes self-rescue extremely difficult, an important consideration for solo seniors.
Q18: What's special about NovaCare?
NovaCare is independently tested by Bureau Veritas (one of the world's largest testing companies, Report BV2500728QN7119), with verified specifications:
- Up to 70 kPa medical-grade suction (independently verified)
- ≥5 L/min airflow tested
- ≥50 kPa air-tightness verified
- IP65 rated (dust and water resistant)
- One-button mechanical design
- One-handed operation
- Reusable (not single-use)
- Self-rescue capable
CE certification (European market) and UKCA certification (UK market) are in progress.
NovaCare's design specifically addresses seniors with medication-induced impairments: even with arthritis, weak grip, or reduced coordination, the one-button mechanism is operable.
Q19: Why does self-rescue capability matter for medication-affected seniors?
Medication-induced choking events often happen when:
- Senior is alone (eating breakfast solo, late-night snack)
- Caregiver is in another room
- During sleep transition (medications cause grogginess)
- After medication peak effect (reduced awareness)
In these scenarios, traditional Heimlich is impossible (alone). LifeVac requires bystander coordination. NovaCare uniquely allows self-rescue:
- Save #156 — Harold B., 78. Choked on steak alone. Self-rescued with NovaCare.
- Save #162 — Dorothy F., 72. Choked on hard candy alone. Self-rescued with NovaCare.
Both seniors had no known dysphagia diagnosis. Both might have had medication-related contributors. Both survived because the device was within reach AND operable solo.
Q20: Should we have both LifeVac AND NovaCare?
For maximum coverage, many families do consider having both:
- LifeVac: For bystander-administered rescue (FDA Authorized)
- NovaCare: For self-rescue capability when alone (Bureau Veritas Tested)
The two devices serve different scenarios. Different households will benefit from different combinations based on their specific situations.
For seniors who live alone (27% of Americans 65+), self-rescue capability is essential — making NovaCare's design particularly relevant.
Section 5: Action Plan for Families (5 Questions)
Q21: What's the first step for adult children?
Within the next 7 days:
- Get complete medication list from your parent (prescriptions + OTC + supplements)
- Ask: "When did you start each one?"
- Ask: "Have you noticed any swallowing changes?"
- Photograph the list
- Search for any AGS Beers Criteria flagged medications
- Schedule consultation with pharmacist
Most pharmacies offer free medication review consultations. Some are covered by insurance.
Q22: What questions should I ask the pharmacist?
Critical questions:
- "Are any of these medications on the AGS Beers Criteria for adults 65+?"
- "What's the cumulative anticholinergic burden of this combination?"
- "Could any of these cause swallowing difficulties or choking risk?"
- "Are there safer alternatives we should discuss with the doctor?"
- "Should we consider deprescribing any of these?"
- "What signs should we watch for?"
Bring written questions. Take notes. Pharmacists are often more thorough than physicians on medication-specific concerns.
Q23: How do I have this conversation with the doctor?
Effective approach:
- Frame as advocacy, not criticism
- Bring specific symptoms documentation
- Reference the AGS Beers Criteria specifically
- Ask about alternatives
- Request swallowing evaluation if symptoms present
- Ask about deprescribing where possible
- Get any changes in writing
Sample script: "I read about the AGS Beers Criteria for medications in adults 65+. Could we review my parent's list to see if any are flagged? I've also noticed some symptoms I'd like to discuss."
Q24: Beyond medication review, what else helps?
Comprehensive prevention strategy:
- Improve oral hygiene — Reduces aspiration pneumonia 50-70%
- Modify diet textures — Smaller bites, softer foods
- Optimize meal posture — Sit upright, stay upright 30 min after
- Reduce mealtime distractions — TV off, slow eating
- Stay hydrated — Reduces medication side effects
- Equipment readiness — Anti-choking device within arm's reach
- Family check-ins — Phone or video during/after meals for solo seniors
Q25: How urgent is this?
For families with seniors on multiple medications, especially the high-risk categories above: urgent.
The risk timeline:
- Subtle dysphagia symptoms: weeks/months ignored
- Silent aspiration: ongoing, undetected
- Aspiration pneumonia: 21% 30-day mortality
- Complete obstruction emergency: 4-minute brain damage window
Most senior families don't address this until after a crisis. Acting before is the difference between a manageable medication adjustment and a potentially fatal emergency.

For Adult Children: A Letter to You
Your parent's medications are saving their life — and possibly endangering it.
Heart medication keeps their heart beating. Antidepressant manages their mood. Sleep aid helps their nights. Bladder medication prevents accidents. Each prescribed for legitimate reasons. Each carrying its own risks.
The question isn't whether they should take medications. The question is whether the cumulative effect — what doctors call "anticholinergic burden" — is creating risks no one has discussed with you.
Here's what I know from working with families:
Most adult children don't review their parent's full medication list. They trust the prescribing physician. They assume someone is monitoring interactions. Often, no one is.
And then someone calls. "Your father aspirated last night. He's in the ICU."
You're left wondering: was there something we could have done?
The answer is yes. Almost always, yes.
The actions:
- Get the complete medication list this week
- Pharmacist review next week
- AGS Beers Criteria check together
- Doctor conversation with specific concerns
- Equipment readiness in their home
- Regular check-ins documenting any changes
The phone call you'll be glad you got: "Mom called. She had a choking moment last night using her usual breakfast. Used the device. She's fine. Going to talk to her doctor about possibly adjusting her medications."
The cost of equipment readiness: $63.98. Free shipping. 90-day guarantee.
→ Get NovaCare for Your Parent — $63.98 single · $119.98 2-pack

The Bottom Line
Medications are essential to senior health management — but the cumulative effects on swallowing function are dramatically underdiscussed. With 35.9% of frail elderly having dysphagia, polypharmacy as a major risk factor, and 17+ medication categories carrying documented dysphagia signals, every adult child should review their parent's medication list against the AGS Beers Criteria.
Equipment readiness — anti-choking device within arm's reach — provides the safety net for when prevention isn't enough.
- ✅ Bureau Veritas Tested (Report BV2500728QN7119)
- ✅ 70 kPa Medical-Grade Suction (Independently Verified)
- ✅ IP65 Rated (Dust & Water Resistant)
- ✅ CE & UKCA Certified
- ✅ 20 Documented Saves in 2026
- ✅ 2 Senior Self-Rescues (#156, #162)
- ✅ Reusable Design (Not Single-Use)
- ✅ Mechanical One-Button (No Batteries)
- ✅ Self-Rescue Capable
- ✅ $63.98 single · $119.98 2-pack
- ✅ Free US Shipping
- ✅ 90-Day Money-Back Guarantee
→ Get NovaCare at novacareus.com
📖 Related: Anti-Choking Device for Seniors: 30 Questions Answered
📖 Related: Anti-Choking Device for Parkinson's Patients
📖 Related: Silent Aspiration in the Elderly
📖 Related: Aspiration Pneumonia in Seniors
📖 Related: NovaCare 2026 Lives Saved Report