


Aspiration Pneumonia in Seniors: Why Most Choking Deaths Aren't From the Choking Itself (2026 Complete Guide)
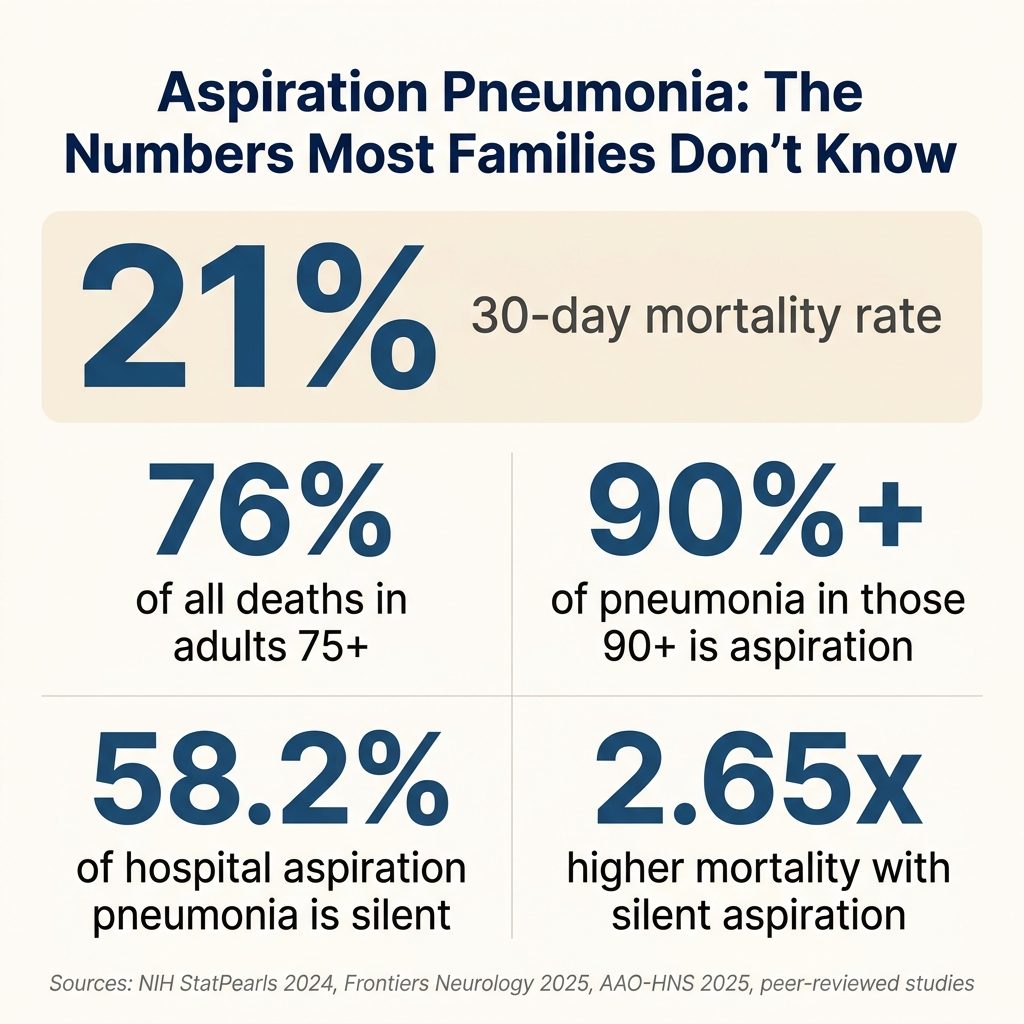
Quick Answer: Most senior deaths "from choking" are actually from aspiration pneumonia — a lung infection that develops 24-72 hours after food, liquid, or saliva enters the lungs. Critical statistics: 21% of aspiration pneumonia cases result in death within 30 days. Adults over 75 account for 76% of all aspiration pneumonia deaths. In Japan, over 90% of pneumonia in adults 90+ is aspiration related. The progression is: silent aspiration → bacteria in lungs → pneumonia → hospitalization → potential death. The NovaCare Anti-Choking Device ($63.98) — Bureau Veritas Tested Class II, Bureau Veritas tested — prevents complete obstruction emergencies that often follow silent aspiration episodes. Save #156 (Harold B., 78, steak, alone) and Save #162 (Dorothy F., 72, hard candy, alone) both prevented what might have become aspiration events.
If your senior parent has been hospitalized with "pneumonia" recently — or twice this year — there's something the doctors may not have told you: it was probably aspiration pneumonia. And aspiration pneumonia isn't bad luck. It's preventable. It's the leading cause of death in nursing homes. And families who understand it have the power to prevent the next episode.
This guide answers what doctors don't usually explain — what aspiration pneumonia actually is, why it kills, and what families can do today.
Section 1: Understanding Aspiration Pneumonia (5 Questions)
Q1: What is aspiration pneumonia?
Aspiration pneumonia is a lung infection caused by inhaling foreign material — food, liquid, saliva, or gastric contents — into the lower airways and lungs. Per StatPearls (NIH 2024), it's a pulmonary infection triggered by entering bacteria-rich oropharyngeal fluids into the lower respiratory tract.
The mechanism:
- Material enters the airway (often via silent aspiration)
- Bacteria from the mouth or stomach reach the lungs
- Lung tissue becomes inflamed
- Infection develops over 24-72 hours
- Pneumonia symptoms emerge (fever, cough, breathing difficulty)
Q2: How is aspiration pneumonia different from regular pneumonia?
The key difference is causation:
- Regular (community-acquired) pneumonia: Caused by airborne pathogens (Streptococcus, viruses, etc.)
- Aspiration pneumonia: Caused by foreign material from one's own body entering the lungs
The treatments differ. The risk factors differ. The prevention differs. Most importantly — aspiration pneumonia is preventable in ways regular pneumonia is not.
Per peer-reviewed Japanese national surveys, in seniors 80-89, about 85% of pneumonia is aspiration-related. In those 90+, the figure exceeds 90%. The takeaway: most senior pneumonia is not "regular" pneumonia.
Q3: How deadly is aspiration pneumonia in seniors?
The numbers are sobering:
| Statistic | Source |
|---|---|
| 21% of cases result in death within 30 days | 2013 study (peer-reviewed) |
| 76% of all aspiration pneumonia deaths are in adults 75+ | Major mortality study |
| 30%+ 30-day mortality in head/neck cancer patients post-treatment | AAO-HNS Bulletin 2025 |
| Over 50% of dysphagia patients experience silent aspirations | StatPearls/NIH 2024 |
| 91.7% of pneumonia patients 70+ have dysphagia | Hospital research |
| Top 3 preventable cause of death in nursing homes | Senior care research |
For context: that 21% 30-day mortality rate is higher than most cancers' equivalent statistic.
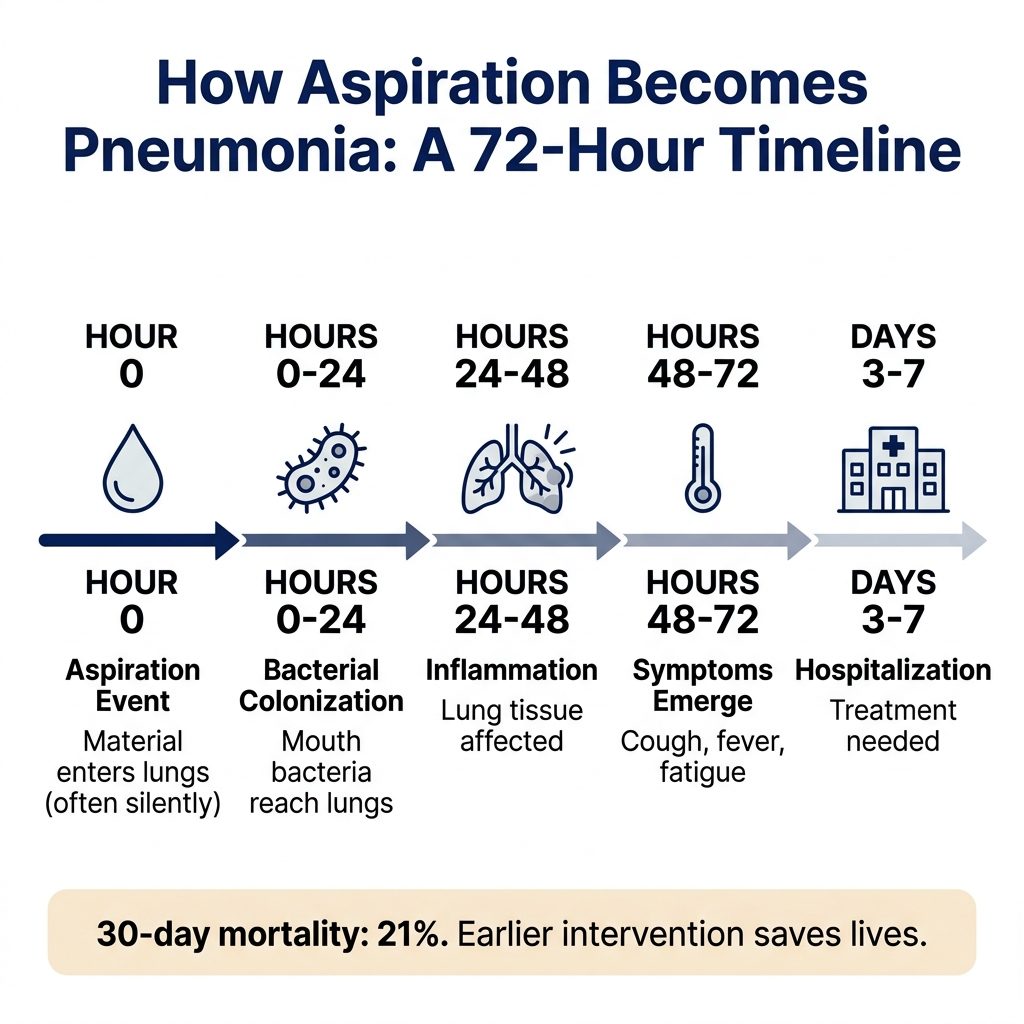
Q4: How quickly does aspiration progress to pneumonia?
The timeline is shorter than most families realize:
- Hour 0: Foreign material enters lungs (often silently)
- Hours 0-24: Bacterial colonization begins
- Hours 24-48: Inflammation increases; lung tissue affected
- Hours 48-72: Symptoms emerge (cough, fever, fatigue)
- Days 3-7: Hospitalization often needed
- Day 30: 21% mortality decision point
Per StatPearls (NIH), patients aspirating after age 80 develop pneumonia in 10% of cases (vs. 5% in those under 80). Even brief aspiration events can be deadly.
Q5: Why are seniors so much more vulnerable?
Several factors compound:
- Weakened cough reflex — Less ability to expel foreign material
- Slower swallowing reflex — Up to 5+ second latency in elderly with repeated pneumonia
- Decreased substance P — Neurotransmitter critical for swallow/cough function
- Lacunar infarction — Small strokes affecting throat protection
- Reduced lung capacity — Less reserve to fight infection
- Frailty and limited mobility — Per StatPearls, more reliable risk indicators than age alone
- Co-morbidities — Heart disease, diabetes, COPD all compound risk
- Medication effects — Sedatives, antipsychotics, opioids reduce protection
- Poor oral hygiene — Higher bacterial load in mouth
Section 2: Who Is at Highest Risk? (5 Questions)
Q6: What conditions dramatically increase aspiration pneumonia risk?
The highest-risk medical conditions:
- Stroke survivors: 30-40% have dysphagia (AAO-HNS)
- Advanced Parkinson's: 60-80% have dysphagia (AAO-HNS) — see our Parkinson's complete guide
- Dementia patients: 72.4% have dysphagia (Frontiers in Neurology 2025)
- Long-term care residents: Over 50% have dysphagia
- Head/neck cancer survivors: Up to 45% have chronic dysphagia, 24% develop aspiration pneumonia within 5 years
- Multiple sclerosis: Common complication
- Huntington's disease: Common complication
- ALS / motor neuron disease: Severely affects swallowing
- Down syndrome adults: Higher prevalence
- GERD patients: Reflux increases aspiration risk
Q7: What about Parkinson's specifically?
Parkinson's deserves special attention. Per AAO-HNS Bulletin 2025, oropharyngeal dysphagia affects 60-80% of those with advanced Parkinson's. And per CDC analysis (2009-2013), Parkinson's has a 2.25% choking death rate — among the highest of any condition.
The symptoms compound:
- Tremor — affects feeding coordination
- Bradykinesia — slow swallowing
- Reduced cough force
- "Off periods" — when medication wears off, swallowing dramatically worsens
- Drooling — saliva pooling in mouth
For Parkinson's families, our dedicated Parkinson's anti-choking guide provides specific recommendations.
Q8: Are nursing home residents at higher risk?
Significantly. Multiple compounding factors:
- Higher prevalence of underlying conditions
- Mealtime supervision challenges
- Texture errors (wrong food consistency)
- Time pressure on staff
- Position errors (not fully upright)
- Communication gaps between SLP recommendations and daily care
Per nursing home research, choking and aspiration pneumonia are among the top three preventable causes of death in long-term care facilities. Families with loved ones in care facilities should specifically ask about aspiration risk protocols.
Q9: How does living alone affect risk?
Living alone presents unique challenges:
- No witness for choking events (silent or otherwise)
- Delayed recognition of pneumonia symptoms
- Self-reporting unreliable — many seniors minimize symptoms
- Emergency response requires self-action
For seniors who live alone, equipment within arm's reach is non-negotiable. Both NovaCare documented senior self-rescues (Save #156, Save #162) occurred to solo-living seniors who saved themselves.
Q10: What about seniors with dental issues or dentures?
Dental health is more important to aspiration pneumonia than most families realize. The connection:
- Dental decay = higher bacterial load in saliva
- Gum disease = active bacterial reservoir
- Loose dentures = impaired chewing + potential aspiration
- Missing teeth = inadequate food breakdown
Per multiple research studies, improved oral hygiene reduces aspiration pneumonia by 50-70%. This is the single highest-impact prevention strategy.
Section 3: Recognizing the Warning Signs (5 Questions)
Q11: What are the early signs of aspiration pneumonia?
Symptoms can be subtle in seniors. Watch for:
- Persistent cough (different from baseline)
- Fever (often low-grade in elderly)
- Shortness of breath
- Increased fatigue
- Chest pain with deep breaths
- Loss of appetite
- Confusion or delirium (often the first sign in elderly)
- Decreased activity level
Critically: per StatPearls, elderly patients with pneumonia often present with non-specific symptoms: general malaise, impaired consciousness, loss of appetite. Many cases are detected only after chest X-ray.
Q12: Why is confusion a key warning sign?
In seniors, the immune response often manifests through cognitive symptoms before respiratory ones. New-onset confusion, increased disorientation, or sudden personality changes can indicate:
- Pneumonia developing
- Sepsis from lung infection
- Hypoxia from impaired breathing
If your previously oriented senior parent suddenly seems confused or disoriented, seek medical evaluation immediately — pneumonia is among the top considerations.
Q13: How do I know if pneumonia is from aspiration vs. regular causes?
Generally, doctors identify aspiration pneumonia based on:
- Risk factors: Stroke, dementia, Parkinson's, etc.
- Clinical presentation: Recent choking incident, observed aspiration
- Chest X-ray patterns: Aspiration typically affects right lower lobe (gravity-dependent)
- Laboratory findings: Anaerobic bacteria in cultures
- Recurrence pattern: Repeated pneumonia in same lung area
If your loved one has had pneumonia, specifically ask the doctor: "Could this have been aspiration pneumonia?" Many primary care doctors don't suggest this evaluation unless prompted.
Q14: What questions should I ask my parent's doctor?
Critical questions to ask:
- "Could this pneumonia have been from aspiration?"
- "Should we get a swallowing evaluation?"
- "Are any of my parent's medications affecting swallowing?"
- "What's the recurrence risk?"
- "Should we see a speech-language pathologist?"
- "What dietary modifications would help?"
- "Is oral hygiene currently adequate?"
- "What signs should I watch for at home?"
Don't accept "just regular pneumonia" without these conversations. Aspiration pneumonia has very different prevention strategies.
Q15: When should I push for hospital evaluation?
Take immediate action if your senior has any of:
- New-onset confusion or disorientation
- Difficulty breathing (especially at rest)
- Fever with cough
- Decreased oxygen saturation (if you have a pulse oximeter)
- Inability to drink fluids
- Chest pain with breathing
- Sudden decrease in activity level
For seniors, aspiration pneumonia can progress from "feeling tired" to ICU-level severity within 48 hours. Earlier evaluation is always better.
Section 4: Treatment & Recovery (5 Questions)
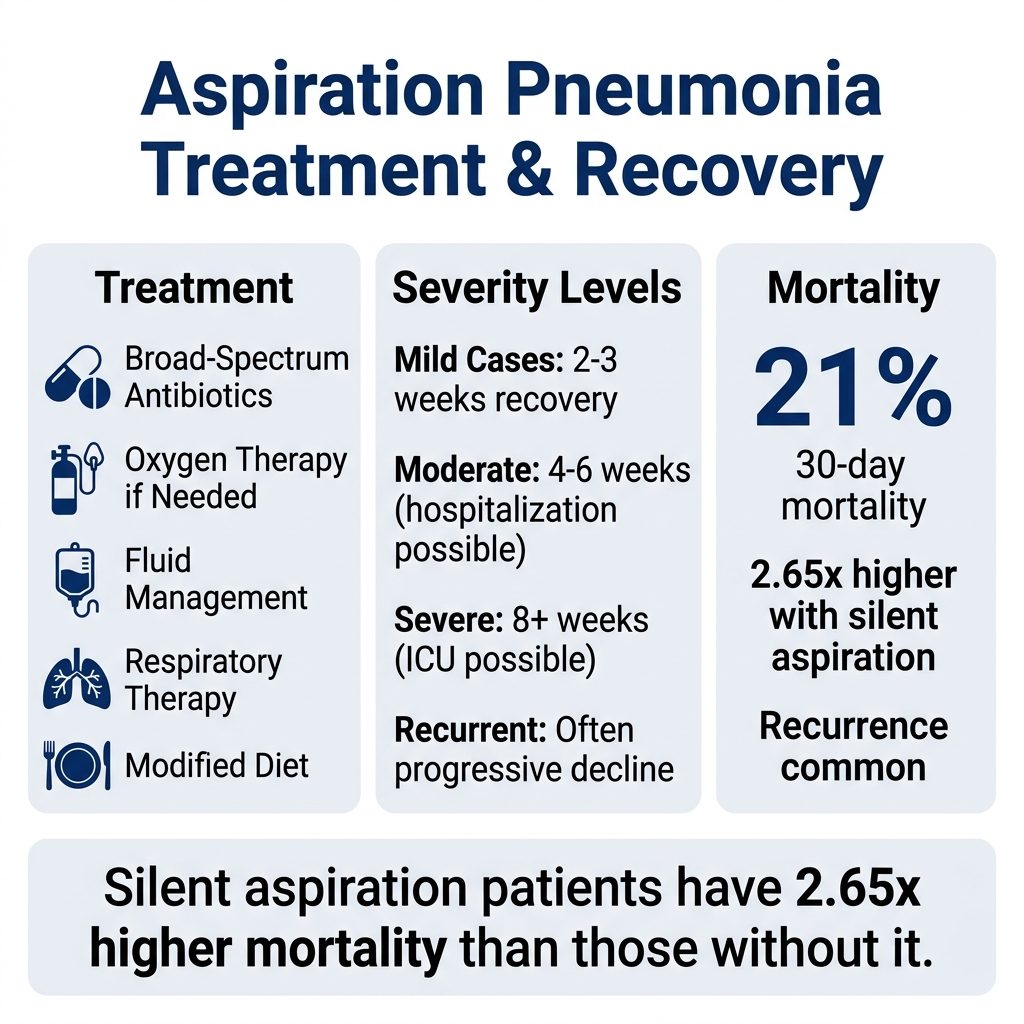
Q16: How is aspiration pneumonia treated?
Treatment generally involves:
- Antibiotics: Often broader spectrum than regular pneumonia (covers anaerobic bacteria)
- Oxygen therapy: If oxygen saturation is low
- Fluid management: IV fluids if dehydration is present
- Respiratory therapy: To clear airways
- Nutrition support: Often modified texture diet during recovery
- Position management: Elevated head of bed
Severe cases may require ICU admission, mechanical ventilation, and prolonged hospitalization. Recovery often takes weeks to months in seniors.
Q17: What about feeding tubes?
Feeding tubes are sometimes considered for seniors with severe dysphagia. The research is increasingly nuanced:
- Pros: Theoretically reduces oral aspiration, ensures nutrition
- Cons: Doesn't prevent aspiration of saliva (still happens), doesn't always extend life, affects quality of life
Per current guidelines, feeding tubes in advanced dementia patients are no longer routinely recommended — they often don't improve survival or quality of life. This is a complex family decision often best made with palliative care guidance.
Q18: How long does recovery take?
Recovery timeline for seniors:
- Mild cases: 2-3 weeks with antibiotics
- Moderate cases: 4-6 weeks; possible hospitalization
- Severe cases: 8+ weeks; possible ICU stay
- Recurrent cases: Often progressive decline
Per peer-reviewed research, silent aspiration patients have 2.65x higher mortality than those without it. Seniors who recover from one aspiration pneumonia event are at significantly elevated risk for another.
Q19: Can a senior fully recover?
Many do, with appropriate intervention:
- Antibiotics resolve immediate infection
- Swallowing therapy can strengthen throat muscles
- Diet modifications reduce future aspiration
- Oral hygiene improvements reduce bacterial load
- Equipment readiness helps prevent emergencies
However, in advanced neurological conditions or extreme frailty, the goal becomes management rather than full recovery. Each subsequent event accelerates decline.
Q20: When should we consider end-of-life decisions?
This conversation deserves serious consideration when:
- Multiple aspiration pneumonia episodes despite intervention
- Advanced dementia with severe swallowing impairment
- Quality of life severely impacted
- Senior expressing desire for comfort care
Many families find peace in knowing they tried prevention thoroughly. Equipment readiness, oral hygiene improvement, and dietary modifications represent the maximum possible action — and even when these don't prevent every event, they extend quality time.
Section 5: Prevention — The Three Pillars (5 Questions)
Q21: What's the most effective prevention strategy?
Research converges on a clear answer: oral hygiene improvement reduces aspiration pneumonia by 50-70%. The mechanism: silent aspiration of saliva is universal in elderly. The bacterial load in that saliva determines pneumonia risk.
Daily oral care protocol:
- Twice-daily teeth brushing (electric toothbrush preferred)
- Daily flossing
- Antiseptic mouthwash if recommended
- Tongue cleaning
- Daily denture cleaning if applicable
- Hydration (reduces bacterial growth)
- Dental cleanings every 6 months
This single intervention has more research support than any other prevention strategy.
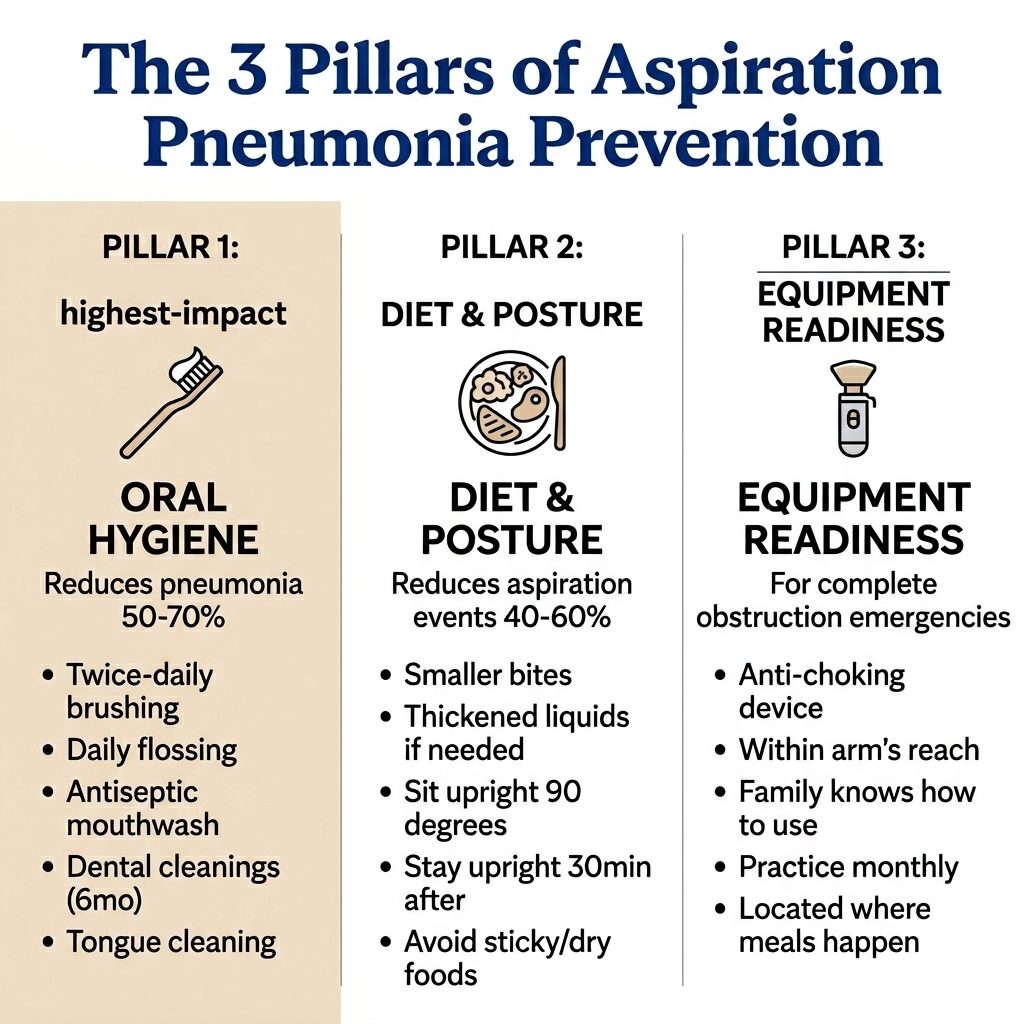
Q22: What dietary modifications reduce risk?
Comprehensive dietary modifications:
- Texture modification: Pureed, minced, or soft foods as appropriate
- Liquid thickening: For seniors who aspirate on thin liquids
- Bite size: Pinky-fingernail size pieces
- Avoid high-risk foods: Hard candy, popcorn, whole nuts, large meat pieces
- Avoid mixed textures: Soup with chunks (smooth or chunky, not mixed)
- Sticky food avoidance: Peanut butter, marshmallows, white bread
- Hydration with meals: Helps food bolus formation
- Slow eating: Set utensils down between bites
For seniors with diagnosed dysphagia, work with a speech-language pathologist for specific recommendations.
Q23: How important is meal posture?
Posture affects safety dramatically:
- Sitting fully upright — 90 degrees, never reclined
- Stay upright 30 minutes after meal — Prevents reflux + aspiration
- Tuck chin slightly when swallowing — Helps redirect food
- Turn head to weaker side for stroke survivors
- Elevate head of bed at minimum 30 degrees when meals must occur in bed
- Take pauses — Don't rush to finish
Position changes alone can reduce aspiration events by 40-60% in some senior populations.
Q24: Should every senior household have an anti-choking device?
Yes — and here's why this is essential, not optional:
Even with perfect oral hygiene, optimal diet, and proper posture, complete obstruction emergencies still occur unpredictably. Both Save #156 (Harold B., 78) and Save #162 (Dorothy F., 72) involved seniors with no prior choking history who suddenly faced complete obstruction emergencies while alone.
NovaCare ($63.98) is specifically designed for senior emergency response:
| Feature | Why It Matters for Seniors |
|---|---|
| One button | Works with arthritis, weak grip, tremors |
| One hand | Self-rescue capable |
| No batteries | Always ready, never needs charging |
| Mechanical | Pure bellows mechanism — won't fail with age |
| Compact (16 cm) | Fits in kitchen drawer or bedside |
| Bureau Veritas Tested | Class II Medical Device |
| Bureau Veritas tested | Up to 70 kPa suction verified (Report BV2500728QN7119) |
| Self-rescue capable | Only major device with this capability |
2-pack ($119.98) recommended for seniors: kitchen + bedside, OR home + adult child's home.
Q25: How do I integrate these prevention strategies?
A practical 30-day implementation plan:
Week 1: Equipment + Awareness
- Order anti-choking device (NovaCare 2-pack)
- Place in kitchen + bedside
- Teach family members basic use
- Practice with included practice mask
Week 2: Oral Hygiene Overhaul
- Schedule dental cleaning
- Improve daily oral care routine
- Address any active dental issues
- Get electric toothbrush if not using
Week 3: Dietary Modifications
- Schedule swallowing evaluation if any concerns
- Review high-risk foods
- Practice smaller bite sizes
- Establish meal posture protocol
Week 4: Medical Conversations
- Discuss aspiration risk with doctor
- Review medications for swallowing effects
- Address any chronic conditions affecting risk
- Establish family check-in protocol
The Connection: Silent Aspiration → Complete Obstruction → NovaCare
Both documented NovaCare senior self-rescues happened to seniors who had likely been silent-aspirating for years without anyone knowing.
Save #156 — Harold B., 78. Widower. Six years of identical Tuesday-night dinners. Always cut his ribeye small. Always chewed slowly. Then one Tuesday a piece — no larger than a dime — went the wrong way. He couldn't cough. He couldn't speak. He had four minutes alone.
Was Harold silently aspirating before that night? Statistical likelihood says yes — at 78, with normal aging, some degree of silent aspiration is nearly universal. He'd just never had a complete obstruction emergency before. The NovaCare his daughter mailed him for Christmas had sat in his drawer for ten weeks. That night, he pressed the button with one hand. The steak came out.
Save #162 — Dorothy F., 72. Watching TV alone. Hard candy. Same situation. No prior choking history. Sudden obstruction. NovaCare on the side table — her daughter had insisted she keep it there.
The lesson: Silent aspiration history (or no history at all) doesn't predict complete obstruction emergencies. They can happen to any senior. Equipment readiness is not optional — it's the difference between a save and a death.
For Adult Children: A Letter to You
Your parent has had pneumonia recently. Maybe more than once.
The doctors gave them antibiotics. They got better. Everyone moved on. Nobody had a serious conversation about why the pneumonia happened.
Here's what they probably didn't tell you: it was likely aspiration pneumonia. The pneumonia wasn't bad luck. It was a signal. And without intervention, it will likely happen again — each time accelerating decline.
The 30-day mortality rate for aspiration pneumonia is 21%. That's higher than most cancers' equivalent statistic. And the recurrence rate without intervention is high.
What you can do:
- Schedule swallowing evaluation — Speech-language pathologist
- Audit medications — Many affect swallowing
- Improve oral hygiene — Reduces pneumonia risk 50-70%
- Modify diet — Smaller bites, softer textures
- Equip the home — Anti-choking device in kitchen + bedside
- Establish protocols — Meal posture, family check-ins
The phone call you don't want is: "Your father is in the ICU with pneumonia. We're not sure he'll make it through the night."
The phone call you'll be glad you got is: "Mom called this morning. She had a choking incident last night, used the device, and called the doctor about a swallowing evaluation."
The difference is preparation. $63.98 starts the equipment side of that preparation.
→ Get NovaCare for Your Parent — $63.98 single · $119.98 2-pack
The 2-pack covers their kitchen + bedside, OR their home + your home for visits.
The Bottom Line

Aspiration pneumonia kills more seniors than house fires, drowning, and accidental poisoning combined. Yet most families discover what it is only after their loved one has already been hospitalized — sometimes only after they've died.
The good news: aspiration pneumonia is preventable. The progression from silent aspiration to complete obstruction to pneumonia to death is well understood, and intervention is possible at every stage.
- ✅ Bureau Veritas Tested Medical Device
- ✅ Bureau Veritas Tested (Report BV2500728QN7119)
- ✅ 20 documented saves in 2026
- ✅ 2 senior self-rescues (#156, #162)
- ✅ 70 kPa Medical-Grade Suction (Independently Verified)
- ✅ IP65 Rated (Dust & Water Resistant)
- ✅ CE & UKCA Certified
- ✅ Reusable Design (Not Single-Use)
- ✅ Mechanical One-Button (No Batteries)
- ✅ Self-Rescue Capable
- ✅ $63.98 single · $119.98 2-pack
- ✅ Free US Shipping
- ✅ 90-Day Money-Back Guarantee
→ Get NovaCare at novacareus.com
📖 Related: Anti-Choking Device for Seniors: 30 Questions Answered
📖 Related: Anti-Choking Device for Parkinson's Patients
📖 Related: NovaCare 2026 Year One Lives Saved Report
📖 Related: Signs of Choking: How to Recognize It in 5 Seconds
📖 Read all saves: NovaCare Life Saved Stories