


AGS Beers Criteria + Choking: 12 Medications Adult Children Should Question (2026 Senior Safety Guide)
Quick Answer: The American Geriatrics Society (AGS) Beers Criteria® is the gold-standard reference for medications adults 65+ should avoid or use with caution. The 2023 edition (most recent) was published May 4, 2023. With more than 90% of older adults using at least one prescription and more than 66% using three or more medications monthly, this list is critical for family safety. Multiple medications on the Beers Criteria carry documented choking and aspiration pneumonia risks. The NovaCare Anti-Choking Device ($63.98) — Bureau Veritas Tested with verified 70 kPa suction — provides emergency response when medication-induced dysphagia leads to choking. LifeVac became FDA De Novo Authorized in March 2026 for bystander rescue. NovaCare specializes in self-rescue scenarios. Most senior households benefit from understanding both options.
Most adult children have never heard of the AGS Beers Criteria. Most primary care physicians don't routinely review it before prescribing. Most pharmacists don't volunteer information about it.
And yet — this list of "Potentially Inappropriate Medications" for adults 65+ identifies dozens of medications that could be silently raising your parent's choking risk. This guide explains everything you need to know.
Section 1: Understanding the AGS Beers Criteria (4 Questions)
Q1: What is the AGS Beers Criteria?
The American Geriatrics Society (AGS) Beers Criteria® for Potentially Inappropriate Medication Use in Older Adults is the most authoritative reference for senior medication safety in the United States.
Origin: Dr. Mark Beers, MD and colleagues at UCLA developed the original list to identify "medications for which potential harm outweighed expected benefit" in nursing home residents. Since 2011, AGS has been the steward of the criteria, producing regular updates.
Most recent update: 2023 edition (published May 4, 2023 in the Journal of the American Geriatrics Society, Volume 71, Issue 7).
The criteria identifies medications across five main categories:
- Potentially inappropriate medications in older adults (general)
- Medications to avoid with certain diseases or syndromes
- Medications to use with caution
- Drug-drug interactions to avoid
- Medications to avoid or dose differently with poor renal function
Q2: Why is this so important for senior safety?
The numbers are sobering:
- 90%+ of older adults use at least one prescription medication
- 66%+ use three or more medications in any given month
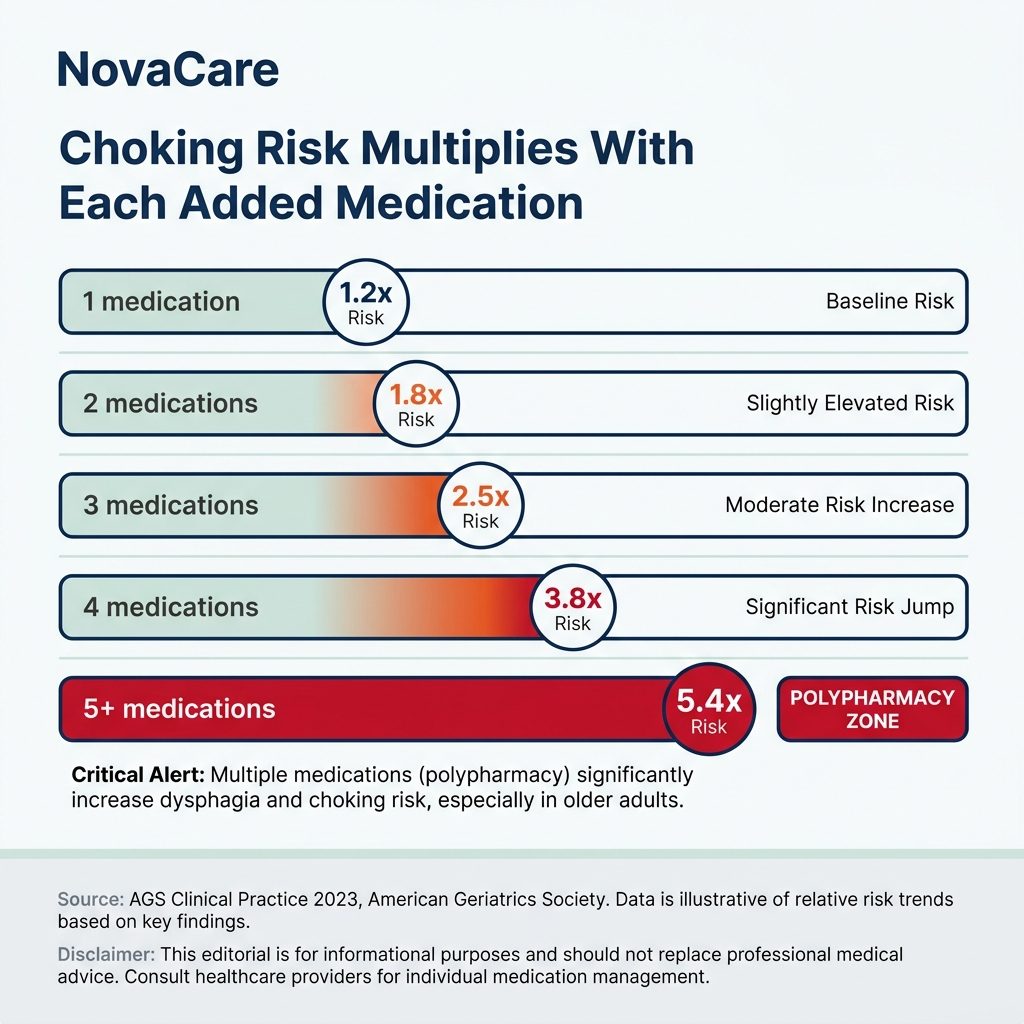
- 30%+ take 5+ medications (polypharmacy)
- 15%+ take 10+ medications
With this level of medication exposure, every senior household needs to understand which medications carry elevated risk for adults 65+.
Per peer-reviewed research, polypharmacy is an independent risk factor for dysphagia (swallowing disorders), with each additional medication increasing risk. Multiple medications on the Beers Criteria carry direct dysphagia/choking risks.
Q3: How do I access the actual Beers Criteria?
The complete 2023 AGS Beers Criteria is available through:
- AGS website: HealthinAging.org (consumer version)
- Journal of American Geriatrics Society: 2023, 71(7), 2052-2081
- Pharmacist consultation: Many pharmacies offer Beers review
- Medicare Annual Wellness Visit: Should include medication review
For comprehensive review, request a Medication Therapy Management consultation — many insurance plans cover this. Pharmacists are typically more thorough than primary care physicians on Beers-specific concerns.
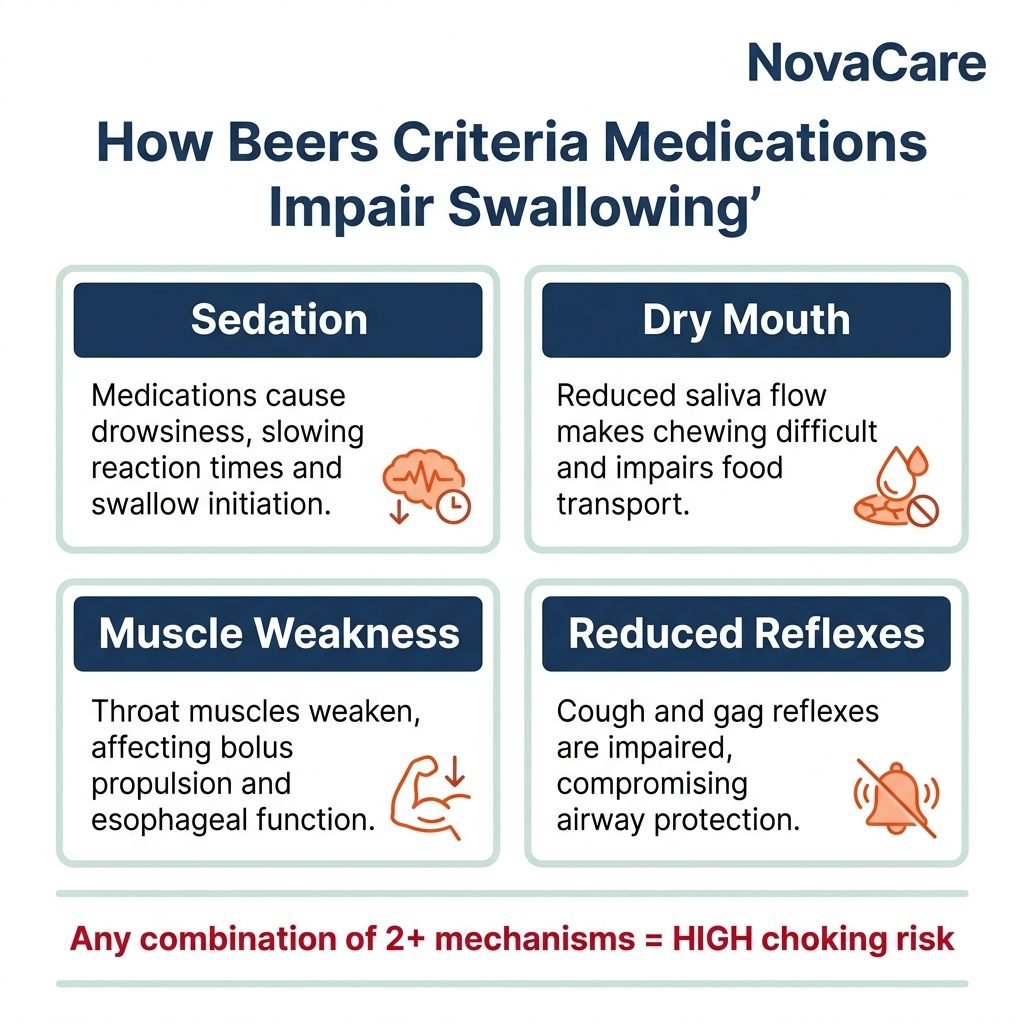
Q4: How does this connect to choking risk?
Many Beers Criteria medications affect swallowing through:
- Anticholinergic effects — Dry mouth, cognitive impairment
- Sedation — Reduced protective reflexes
- Dopamine blocking — Swallowing coordination impairment
- Cumulative anticholinergic burden — Combined medications compound risk
Per peer-reviewed pharmacovigilance research using the FDA Adverse Event Reporting System (FAERS) database, dopamine-blocking drugs (especially antipsychotics) are primary contributors to medication-related aspiration pneumonia risk in elderly populations.
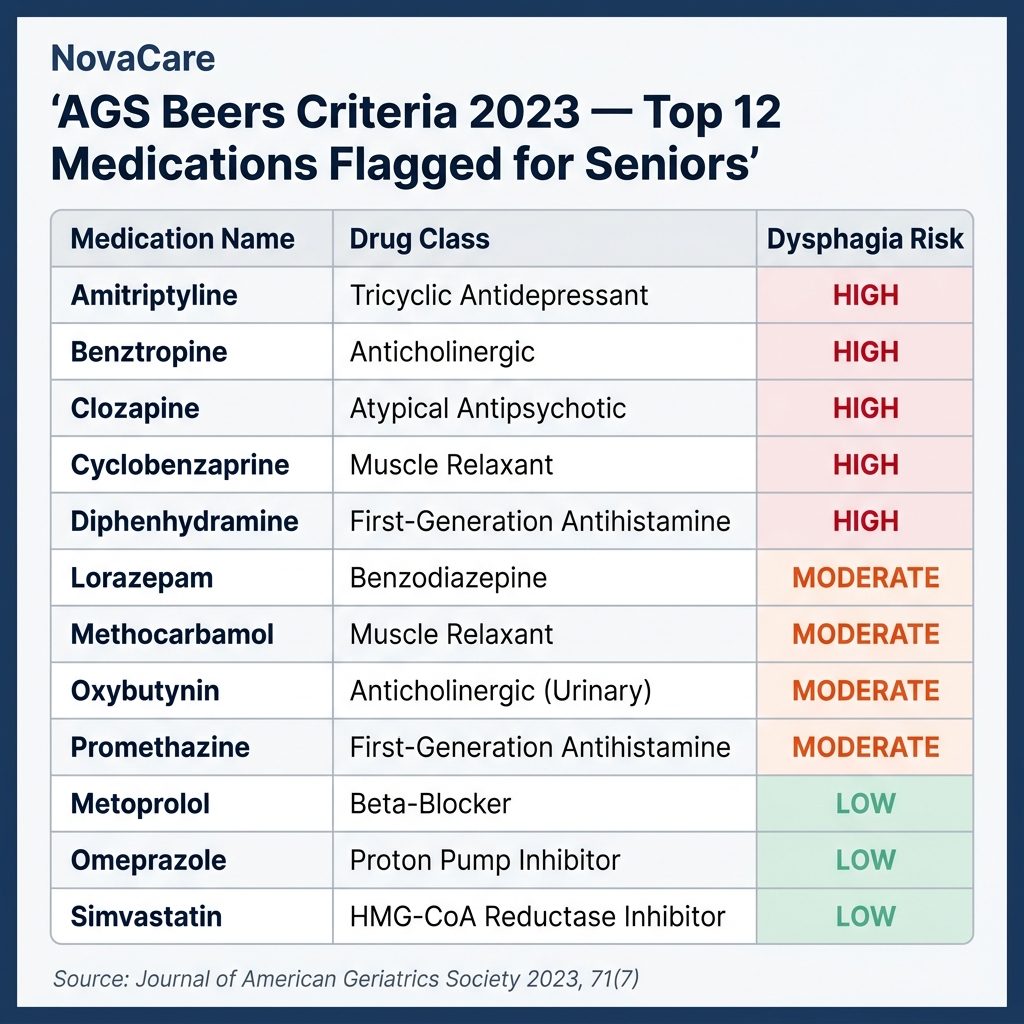
Section 2: 12 Beers Criteria Medications That Affect Choking Risk (12 Questions)
Q5: Medication #1 — Antipsychotics (Aripiprazole, Risperidone, Olanzapine, Quetiapine, Haloperidol)
Beers Status: Avoid in adults 65+, especially for dementia behavioral symptoms (Black Box warning)
Brand names: Abilify, Risperdal, Zyprexa, Seroquel, Haldol
Choking mechanism:
- Block dopamine pathways involved in swallowing coordination
- Per CDC data, schizophrenia patients have 2.66% choking death rate
- Dose-dependent effect
- Both first-generation (Haldol) and second-generation (Abilify, Zyprexa) carry risk
Why prescribed for elderly: Often for dementia behavioral symptoms (off-label, despite Beers warning)
Action: If parent on antipsychotics for dementia, urgent discussion needed about alternatives. The Beers Criteria specifically warns against this use.
Q6: Medication #2 — Benzodiazepines (Diazepam, Alprazolam, Lorazepam, Clonazepam)
Beers Status: Avoid for chronic use in adults 65+
Brand names: Valium, Xanax, Ativan, Klonopin
Choking mechanism:
- Sedation reduces protective swallowing reflexes
- Particularly dangerous if drowsy during meals
- Can cause cognitive impairment affecting eating awareness
- Risk highest at peak effect timing
Why prescribed: Anxiety, insomnia, panic disorders
Action: Consider tapering with physician supervision. SSRIs may be safer for long-term anxiety in elderly.
Q7: Medication #3 — Z-drugs (Zolpidem, Eszopiclone, Zaleplon)
Beers Status: Avoid chronic use; if used, limit to less than 90 days
Brand names: Ambien, Lunesta, Sonata
Choking mechanism:
- Sedation continues into morning hours
- Particularly problematic for early breakfast
- Reduced cough reflex during sleep transition
- Disrupts swallowing coordination
Why prescribed: Insomnia
Action: Discuss alternatives like cognitive behavioral therapy for insomnia (CBT-I), sleep hygiene improvements, or low-dose melatonin.
Q8: Medication #4 — Tricyclic Antidepressants (Amitriptyline, Nortriptyline, Doxepin)
Beers Status: Avoid in adults 65+ (high anticholinergic effects, sedation)
Brand names: Elavil, Pamelor, Sinequan
Choking mechanism:
- Strong anticholinergic effects → dry mouth
- Sedation → reduced reflexes
- Often prescribed for sleep (low dose)
- Combines dangerously with other medications
Why prescribed: Depression, neuropathic pain, sleep, migraines
Action: SSRIs and SNRIs are typically safer for elderly. For pain, topical alternatives often work.
Q9: Medication #5 — Anticholinergic Antihistamines (Diphenhydramine, Hydroxyzine, Chlorpheniramine)
Beers Status: Avoid in adults 65+ (highly anticholinergic, drowsy)
Brand names: Benadryl, ZzzQuil, Tylenol PM, Sominex, Atarax
Choking mechanism:
- Strong anticholinergic → severe dry mouth
- Sedation effects
- Cognitive impairment risk
- Often combined with other medications without realization
Why used: Allergies, sleep aid, anxiety (OTC and prescription)
Action: Newer antihistamines (loratadine/Claritin, cetirizine/Zyrtec) are safer alternatives. For sleep, address underlying causes.
Critical concern: Many seniors don't realize "PM" formulations of OTC pain relievers contain diphenhydramine. Tylenol PM = Tylenol + Benadryl.
Q10: Medication #6 — Anticholinergic Bladder Medications (Oxybutynin, Tolterodine, Solifenacin)
Beers Status: Use with caution in adults 65+; avoid in dementia
Brand names: Ditropan, Detrol, Vesicare
Choking mechanism:
- Strong anticholinergic → dry mouth
- Cognitive effects
- Cumulative burden if combined with other anticholinergics
- May worsen dementia symptoms
Why prescribed: Overactive bladder, urinary incontinence
Action: Mirabegron (Myrbetriq) is a newer alternative with less anticholinergic burden. Behavioral therapy first-line.
Q11: Medication #7 — Skeletal Muscle Relaxants (Cyclobenzaprine, Methocarbamol, Carisoprodol)
Beers Status: Avoid in adults 65+ (highly anticholinergic, sedation, fracture risk)
Brand names: Flexeril, Robaxin, Soma
Choking mechanism:
- Anticholinergic effects
- Sedation
- Muscle weakness (including throat)
- Fall risk also increased
Why prescribed: Back pain, muscle spasms
Action: Topical NSAIDs, physical therapy, gabapentin for nerve pain — safer alternatives.
Q12: Medication #8 — Long-acting Sulfonylureas (Glyburide, Chlorpropamide)
Beers Status: Avoid in adults 65+ (severe hypoglycemia risk)
Brand names: Diabeta, Diabinese
Choking mechanism:
- Hypoglycemia → confusion → impaired eating safety
- Severe lows can cause loss of consciousness during meals
- Risk of aspiration during hypoglycemic episodes
Action: Newer diabetes medications (DPP-4 inhibitors, GLP-1 agonists) safer for elderly.
Q13: Medication #9 — Opioid Pain Medications (Long-term)
Beers Status: Use with caution; avoid combination with benzodiazepines
Brand names: OxyContin, Vicodin, Norco, Tramadol
Choking mechanism:
- Sedation reduces protective reflexes
- Reduced cough strength
- Dry mouth
- Constipation can affect swallowing comfort
- Combined with other CNS depressants = severe risk
Action: Multimodal pain management. Topical NSAIDs, acetaminophen, physical therapy.
Q14: Medication #10 — Proton Pump Inhibitors (Long-term)
Beers Status: Avoid scheduled use beyond 8 weeks unless specific indication
Brand names: Prilosec, Nexium, Prevacid, Protonix
Choking mechanism:
- Long-term use associated with increased pneumonia risk
- Reduces protective gastric acid (more aspiration concerns)
- Can cause vitamin/mineral deficiencies affecting muscle function
Why prescribed: GERD, peptic ulcer disease
Action: Step-down therapy, lifestyle modifications, H2 blockers for some indications.
Q15: Medication #11 — Diphenhydramine for Parkinson's (Trihexyphenidyl, Benztropine)
Beers Status: Avoid for Parkinson's in adults 65+
Brand names: Artane, Cogentin
Choking mechanism:
- Anticholinergic effects compound dysphagia already present in Parkinson's
- 60-80% of advanced Parkinson's patients have dysphagia (AAO-HNS)
- Cumulative anticholinergic burden severe
Action: Modern Parkinson's medications (carbidopa-levodopa, dopamine agonists) generally safer. Anticholinergic Parkinson's drugs largely outdated.
Q16: Medication #12 — Combination of Three Or More CNS-Active Medications
Beers Status: Avoid 3+ CNS-active medications (high fall and choking risk)
This isn't one medication but a combination warning:
- Antipsychotics + antidepressants + sleep aids
- Benzodiazepines + opioids + muscle relaxants
- Antihistamines + bladder medications + tricyclics
The cumulative anticholinergic burden is what kills. The Beers Criteria specifically warns about this in 2023 update.
Action: Comprehensive medication review. Pharmacist Medication Therapy Management consultation.
Section 3: How to Conduct a Medication Review (5 Questions)
Q17: How do I get my parent's complete medication list?
Step-by-step process:
- Ask parent directly — Have them gather everything
- Inspect medicine cabinet — Often more than they remember
- Check refrigerator — Some medications stored there
- Pharmacy records — Request printout (with their permission)
- Doctor records — Each provider may have different list
- Don't forget OTC — Vitamins, supplements, herbal remedies
- Photograph everything — Pill bottles tell important stories
Common surprises:
- Multiple doctors prescribing without coordination
- Medications "from years ago" still being taken
- OTC sleep aids combined with prescription sedatives
- Supplements interacting with prescriptions

Q18: How do I conduct the AGS Beers cross-reference?
Two approaches:
DIY approach:
- Visit HealthinAging.org for consumer-friendly Beers info
- List each medication
- Search [medication name] + "AGS Beers Criteria"
- Note which medications are flagged
- Especially watch for: anticholinergic, sedative, antipsychotic categories
Professional approach (recommended):
- Schedule pharmacist Medication Therapy Management consultation
- Bring complete list (including OTC)
- Ask: "Are any of these on AGS Beers Criteria?"
- Ask: "What's the cumulative anticholinergic burden?"
- Get written summary
Q19: What questions should I ask the doctor?
Critical conversation points:
- "I'd like to review which medications are appropriate for adults 65+"
- "Could we discuss the AGS Beers Criteria in relation to mom's medications?"
- "Are there safer alternatives we should consider?"
- "What's the deprescribing protocol if we want to taper?"
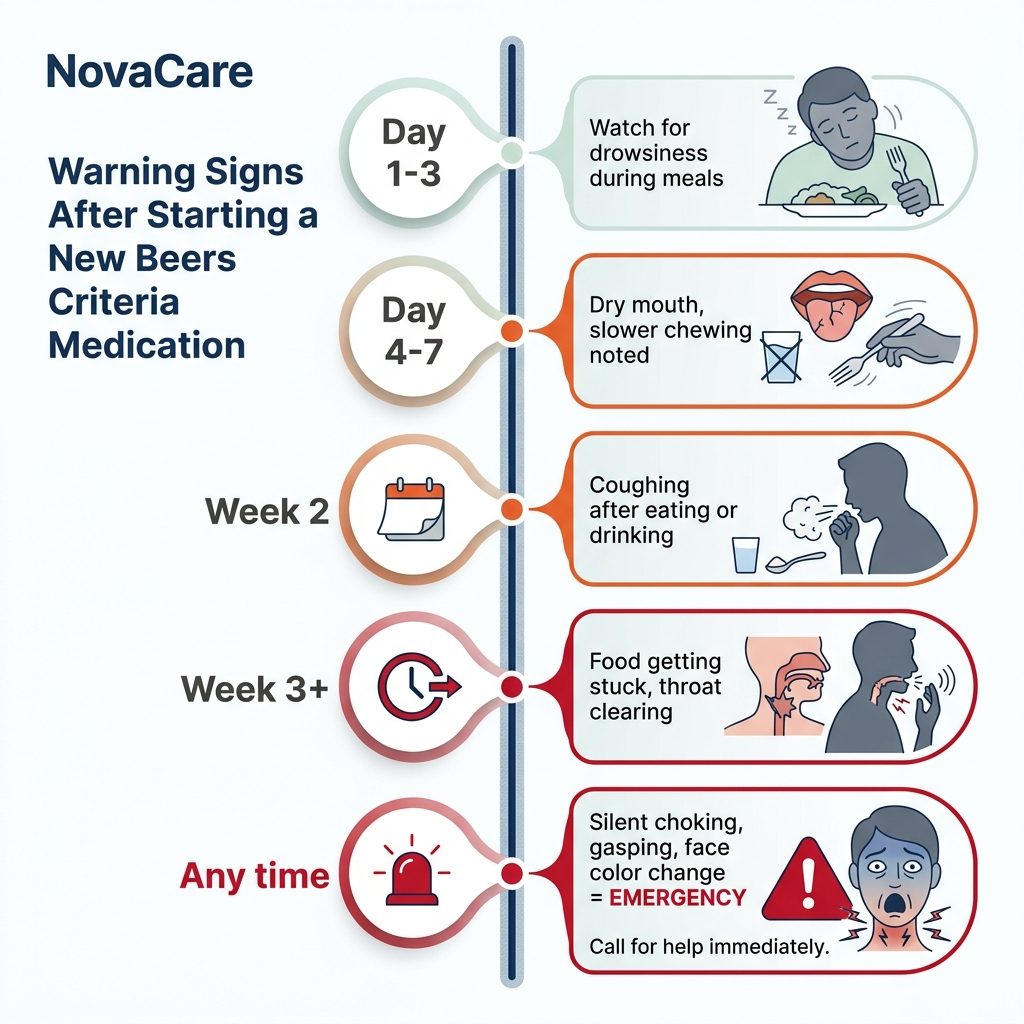
- "How would we know if dysphagia symptoms appear?"
- "Should we get a swallowing evaluation?"
- "What signs warrant immediate concern?"
Bring documentation. Take notes. Don't accept "everything's fine" without specific Beers cross-reference.
Q20: What if doctor dismisses concerns?
If primary care physician doesn't engage with Beers Criteria seriously:
- Get geriatrician referral — Specialists in elderly care
- Pharmacist consultation — Direct booking, no referral needed
- Switch primary care — Find geriatric-aware physician
- Document concerns in writing — Patient portal messages
- Get second opinion — Especially before significant medication changes
You're the senior's advocate. Don't accept dismissive treatment when their safety is at stake.
Q21: What is "deprescribing" and is it safe?
Deprescribing = systematic process of dose reduction or stopping medications that may no longer be appropriate or beneficial.
Done correctly, deprescribing:
- Reduces side effect burden
- Improves quality of life
- Lowers cost
- Reduces choking risk
- Reduces fall risk
Critical: NEVER stop medications without physician supervision. Especially:
- Long-term benzodiazepines (severe withdrawal)
- Antidepressants (discontinuation syndrome)
- Antipsychotics (rebound symptoms)
- Cardiac medications (life-threatening if stopped)
- Diabetes medications (glucose control)
Tapering is supervised, gradual, and may take weeks to months.
Section 4: Equipment Comparison for Medication-Affected Seniors (4 Questions)
Q22: How do anti-choking devices compare for medication-affected seniors?
For families managing medication-related choking risks, equipment matters. The major options:
| Device | Status | Use Case |
|---|---|---|
| LifeVac | FDA De Novo Authorized (March 2026) | Bystander rescue, single-use |
| NovaCare | Bureau Veritas Tested | Self-rescue, reusable |
| Sonmol | Various | Wall-mounted, 5-step |
| Dechoker | Multiple FDA actions | Tube-based |
Q23: Why does self-rescue capability matter for medication-affected seniors?
Medication-induced choking events frequently happen when:
- Senior is alone (early morning before family wakes)
- After medication peak effect (drowsy)
- During sleep transitions
- Caregiver in other room
- 27% of Americans 65+ live alone
In these scenarios:
- Heimlich is impossible — Requires bystander
- LifeVac is difficult — Designed for bystander use
- NovaCare is uniquely designed — Self-rescue capable
Documented self-rescue cases:
- Save #156 — Harold B., 78. Choked on steak, alone. Self-rescued.
- Save #162 — Dorothy F., 72. Choked on hard candy, alone. Self-rescued.
Both seniors had no known dysphagia diagnosis. Both might have had medication contributors. Both survived because the device was operable solo.
Q24: What about LifeVac for these scenarios?
LifeVac became the first FDA De Novo Authorized anti-choking device on March 4, 2026, classified as Class II for second-line treatment.
LifeVac advantages:
- FDA Authorization (Class II)
- Multiple peer-reviewed studies
- 5,500+ documented saves globally
- Multiple mask sizes for ages
LifeVac considerations for medication-affected seniors:
- Single-use (must replace after use)
- Two-handed plunger operation
- Difficult to self-administer
- Best with capable bystander present
For households where senior is rarely alone, LifeVac may be excellent. For solo seniors, NovaCare's self-rescue design fills a different need.
Q25: Should families have both devices?
For maximum coverage, having both devices makes sense:
- LifeVac — When capable bystander present (FDA Authorized)
- NovaCare — When senior is alone (Bureau Veritas Tested, self-rescue)
The two devices serve different scenarios. Different households benefit from different combinations based on their specific situations:
- Senior lives alone → NovaCare critical, LifeVac optional
- Senior with full-time caregiver → LifeVac primary, NovaCare backup
- Senior splits time → Both essential
- Senior in family home → Both for different scenarios
For multi-location coverage, NovaCare's 2-pack ($119.98) provides cost-effective dual-location safety.

For Adult Children: A Letter to You
Your parent has 12 medications. Maybe more.
Each prescribed by a different specialist. None of them talking to each other. None of them reviewing the AGS Beers Criteria. None of them asking about cumulative anticholinergic burden.
And your parent? They trust their doctors. They take their pills. They notice — but don't connect — the dry mouth, the morning grogginess, the occasional cough during meals. "It's just aging," they tell themselves.
It might not be just aging. It might be medications interacting in ways no single doctor sees.
The Beers Criteria exists because experts worked to identify exactly this problem. Yet most families never hear about it. Most prescriptions get written without it. Most pharmacy reviews don't reference it.
You can change this. This week:
- Get your parent's complete medication list
- Request a Medication Therapy Management consultation with their pharmacist
- Specifically ask about AGS Beers Criteria flags
- Ask about cumulative anticholinergic burden
- Schedule swallowing evaluation if any concerns
- Have anti-choking equipment within reach
The conversation might be uncomfortable. The action is essential.
Save #156's daughter sent her father a NovaCare device for Christmas. He kept it in his kitchen drawer for ten weeks. Then one Tuesday — after years on multiple medications including ones from the Beers list — a piece of steak went the wrong way. He used the device. He survived.
That's what equipment readiness looks like in practice.
→ Get NovaCare for Your Parent — $63.98 single · $119.98 2-pack

The Bottom Line
The AGS Beers Criteria is among the most authoritative resources for senior medication safety in the United States. Yet most families never hear about it, and most primary care physicians don't routinely reference it. Multiple Beers-flagged medications carry choking and aspiration risks through anticholinergic effects, sedation, dopamine blocking, or cumulative burden.
For families with seniors on 5+ medications: comprehensive review against the Beers Criteria is urgent.
- ✅ Bureau Veritas Tested (Report BV2500728QN7119)
- ✅ 70 kPa Medical-Grade Suction (Independently Verified)
- ✅ IP65 Rated (Dust & Water Resistant)
- ✅ CE & UKCA Certified
- ✅ 20 Documented Saves in 2026
- ✅ 2 Senior Self-Rescues (#156, #162)
- ✅ Reusable Design (Not Single-Use)
- ✅ Mechanical One-Button (No Batteries)
- ✅ Self-Rescue Capable
- ✅ $63.98 single · $119.98 2-pack
- ✅ Free US Shipping
- ✅ 90-Day Money-Back Guarantee
→ Get NovaCare at novacareus.com
📖 Related: Anti-Choking Device for Seniors: 30 Questions Answered
📖 Related: Anti-Choking Device for Parkinson's Patients
📖 Related: Silent Aspiration in the Elderly
📖 Related: Aspiration Pneumonia in Seniors
📖 Related: NovaCare 2026 Lives Saved Report